Printable Medical Clearance Form For Dental Treatment
Printable Medical Clearance Form For Dental Treatment - Up to 40% cash back the document is a medical clearance form for dental treatment, requesting evaluation of a patient's medical history and any special considerations from their. Sign, print, and download this pdf at printfriendly. Dentist name (please print) patient signature date physicians: Evaluate this patient's medical history and advise us of any special considerations that should be made. Please evaluate this patient's medical. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: It ensures that the patient's medical history is reviewed by a physician. Fill in your personal information accurately, including your name, date of birth, and. Download a free printable dental clearance form template. Please complete the section below. A typical medical clearance form for dental treatment includes several key components: Sign, print, and download this pdf at printfriendly. Fill in your personal information accurately, including your name, date of birth, and. Up to $50 cash back obtain the dental clearance form from your dentist or healthcare provider. The patient has indicated the following medical conditions: Medical clearance for dental treatment date: Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Name, birth date, and contact details. Our mutual patient (listed above) is scheduled for dental hygiene and/or dental treatment appointment. We appreciate your assistance in providing optimum care for this patient. A typical medical clearance form for dental treatment includes several key components: Up to 40% cash back the document is a medical clearance form for dental treatment, requesting evaluation of a patient's medical history and any special considerations from their. Does the patient require antibiotic. Medical clearance for dental treatment date: This form is essential for obtaining medical clearance prior. Dentist name (please print) patient signature date physicians: View the medical clearance for dental treatment form in our collection of pdfs. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Up to $50 cash back obtain the dental clearance form from your dentist or healthcare provider. Our mutual patient, _____ is scheduled for dental. A typical medical clearance form for dental treatment includes several key components: Evaluate this patient's medical history and advise us of any special considerations that should be made. Complete this form to help your dentist. Our mutual patient, _____ is scheduled for dental treatment. The patient has indicated the following medical conditions: To begin, download the printable dental clearance form template from our website. Please complete the section below. Perfect for documenting patient details, medical history, and dental history. Up to $50 cash back obtain the dental clearance form from your dentist or healthcare provider. View the medical clearance for dental treatment form in our collection of pdfs. Our mutual patient, _____ is scheduled for dental treatment. Please complete the section below. Patient indicates a medical concern of: This form is essential for obtaining medical clearance prior to dental treatment. Up to 40% cash back the document is a medical clearance form for dental treatment, requesting evaluation of a patient's medical history and any special considerations from their. Complete this form to help your dentist. Perfect for documenting patient details, medical history, and dental history. In order for us to deliver safe and efficient dental treatment while being aware of patient’s medical condition, i would like to request a brief written medical clearance to ensure that any of the. Name, birth date, and contact details. Up to 40%. Complete this form to help your dentist. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: We appreciate your assistance in providing optimum care for this patient. This document collects crucial information about a patient’s dental and medical history, ensuring. Our mutual patient (listed above) is scheduled for dental hygiene and/or dental treatment appointment. Complete this form to help your dentist. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: View the medical clearance for dental treatment form in our collection of pdfs. Fill in your personal information accurately, including your name, date of birth, and. Please evaluate this patient's medical. Download a free printable dental clearance form template. Our mutual patient (listed above) is scheduled for dental hygiene and/or dental treatment appointment. This form is essential for obtaining medical clearance prior to dental treatment. Please complete the section below. This document collects crucial information about a patient’s dental and medical history, ensuring. This form is essential for obtaining medical clearance prior to dental treatment. Evaluate this patient's medical history and advise us of any special considerations that should be made. Complete this form to help your dentist. Up to 40% cash back the document is a medical clearance form for dental treatment, requesting evaluation of a patient's medical history and any special. Patient indicates a medical concern of: Please evaluate this patient's medical. Our mutual patient, as noted above, is scheduled for dental treatment at our office. Our mutual patient (listed above) is scheduled for dental hygiene and/or dental treatment appointment. Fill in your personal information accurately, including your name, date of birth, and. To begin, download the printable dental clearance form template from our website. This document collects crucial information about a patient’s dental and medical history, ensuring. Download a free printable dental clearance form template. This form is essential for obtaining medical clearance prior to dental treatment. Complete this form to help your dentist. Perfect for documenting patient details, medical history, and dental history. Medical clearance for dental treatment date: Please complete the section below. Sign, print, and download this pdf at printfriendly. In order for us to deliver safe and efficient dental treatment while being aware of patient’s medical condition, i would like to request a brief written medical clearance to ensure that any of the. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician:
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs

Fillable Online Medical Clearance for Dental Treatment Drs. Allison
Clean Minimalist Dental Clearance Consent Form Venngage
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs

Dental Clearance Form & Example Free PDF Download

Printable Medical Clearance Form For Dental Treatment DocTemplates

Printable Medical Clearance Form For Dental Treatment
FREE 31+ Medical Clearance Forms in PDF MS Word

Printable Dental Clearance Form For Surgery
Printable Dental Clearance Form For Surgery
A Typical Medical Clearance Form For Dental Treatment Includes Several Key Components:
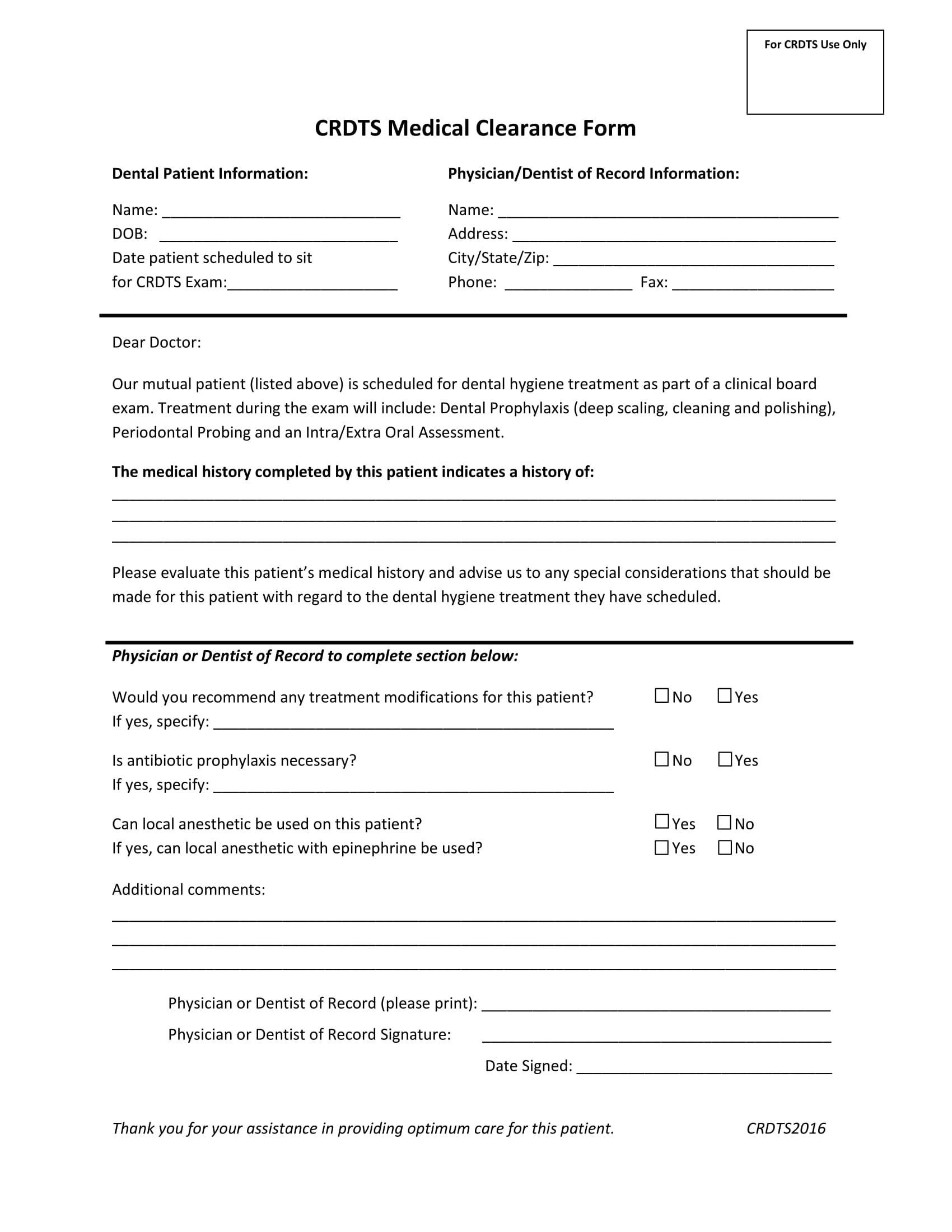
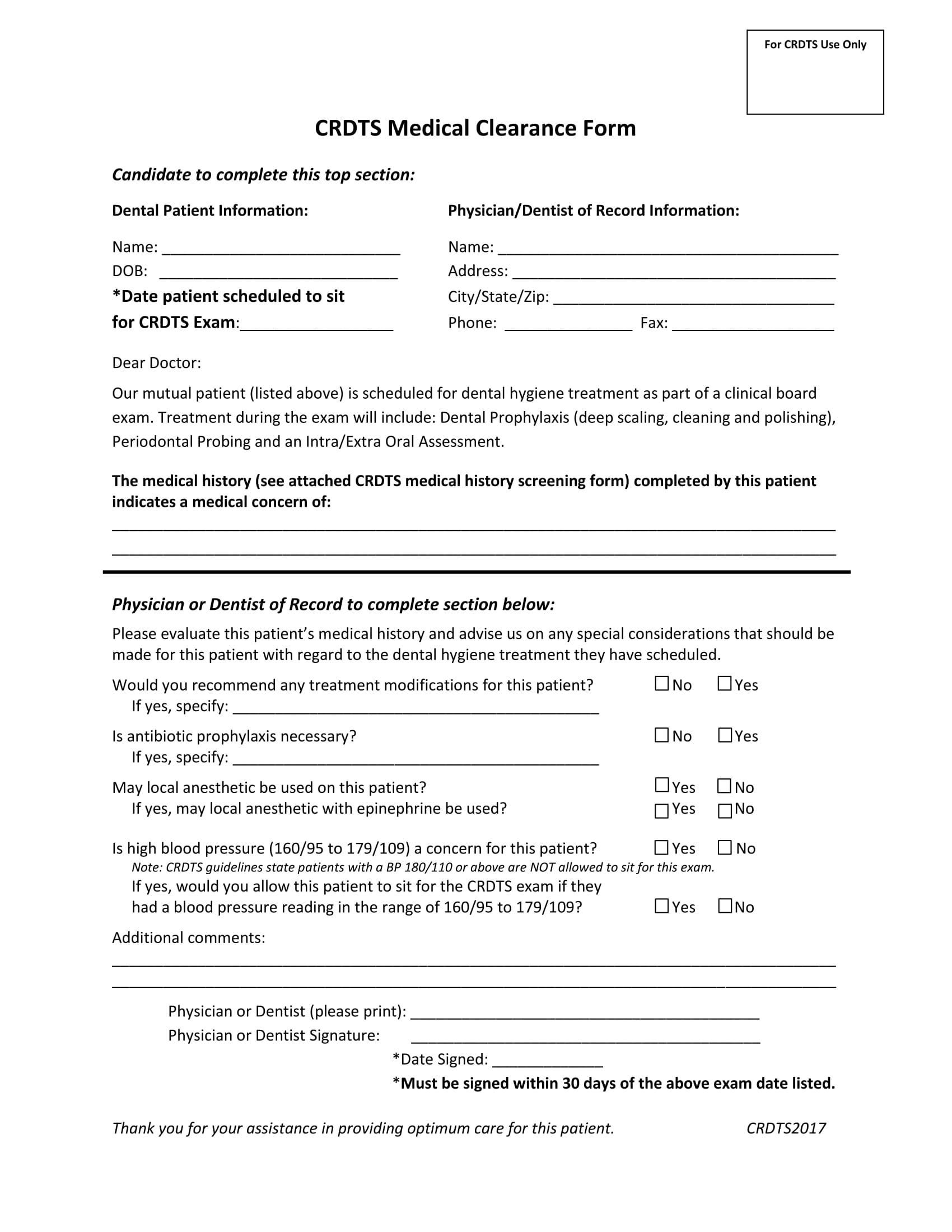
Dentist Name (Please Print) Patient Signature Date Physicians:
Please Ensure That Your Medical Provider Completes This Form And Returns It To Your Dental Office Before Your Scheduled Dental Procedure.
Our Mutual Patient, _____ Is Scheduled For Dental Treatment.
Related Post: